Operations at the Brazilian Populational-Based Cancer Registry, São Paulo City: A Conversation with Fernanda Michels


NAACCR Associate Director, Stephanie Hill, sat down with NAACCR Program Manager for Data Quality and Integration, Dr. Fernanda Michels, to talk about how she became involved in the international cancer registry community and how it’s shaped her work in cancer surveillance.
Stephanie Hill: In your role at NAACCR, you do a lot of work with the international community. What drew you to that aspect of cancer surveillance?
Fernanda Michels: I’m originally from Brazil, and I began my career working at the São Paulo Population-Based Cancer Registry (SP-PBCR) from 2008 to 2013. In 2012, I continued working remotely after moving to the U.S. That early experience gave me a deep understanding of how cancer registries operate in different settings, especially under resource constraints. Since then, I’ve remained passionate about supporting international collaboration and improving cancer surveillance globally.
SH: Has there always been a population-based cancer registry in São Paulo?
FM: São Paulo is the largest city in the Southern Hemisphere, with over 11 million residents according to the 2024 census. The SP-PBCR was initially structured in January 1963 as a pilot project and officially launched in January 1969. It became part of the Department of Epidemiology at the University of São Paulo’s School of Public Health. The registry played a key role in producing high-quality cancer data for research, public health, and international reporting for many decades.
SH: Wow, that’s older than some U.S. registries. What was your role at the SP-PBCR?
FM: I was the director with support from the Epidemiology Professor from the University of São Paulo’s School of Public Health, Dr. Maria do Rosario Dias de Oliveira Latorre. I was responsible for overseeing and coordinating key aspects of registry operations, including data collection, quality control, and case verification. I worked closely with our data collectors and IT team to ensure data consistency, manage linkage procedures, and resolve duplicates.
SH: How were registry operations different at the SP-PBCR from in the U.S.?
FM: The SP-PBCR used a mixed model of active and passive data collection across a wide network of 301 data sources, including hospitals, clinics, pathology labs, death investigation services, and hospital-based registries. Of these, 245 were visited regularly by trained data collectors. In contrast, most U.S. registries rely more heavily on electronic reporting and automated systems. Our processes in São Paulo were often more manual and labor-intensive, requiring routine in-person visits and substantial staff time for data validation and linkage.
Another major difference is the amount of data collected—SP-PBCR collected significantly fewer data items than U.S. registries <Figure 1>. The focus was on a core set of high-priority variables, which made the process more manageable given the limited resources, but also meant fewer details were available for analysis compared to U.S. datasets.
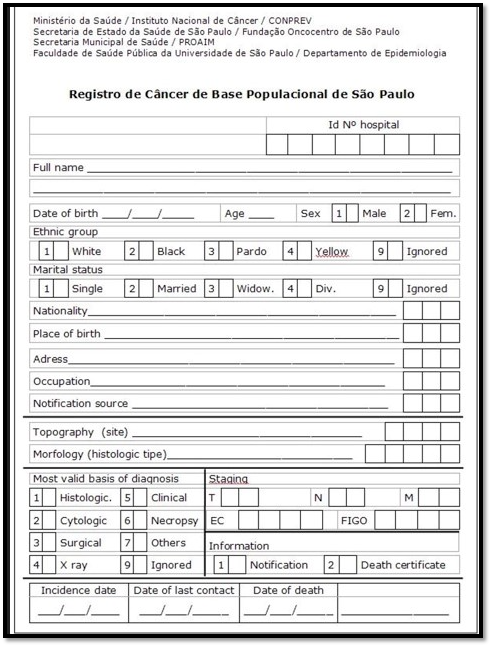
Figure 1
SH: What kinds of challenges did the SP-PBCR face?
FM: One of the biggest challenges was inconsistent funding, which led to interruptions in data collection during different periods. Unfortunately, due to prolonged funding shortages, the registry is currently closed. Despite that, the SP-PBCR maintained high-quality operations for decades, and the lessons from that experience continue to inform registry development in other low- and middle-income countries.
SH: How did your work with the SP-PBCR prepare you to work with registries in the US and other countries?
FM: Working with limited resources taught me how to innovate and prioritize data quality even under constraints. I gained hands-on experience in every part of the cancer registration process—from data abstraction and duplication checks to software development and death clearance procedures. That background has been incredibly valuable in my current role, where I help registries across the globe implement practical and sustainable solutions, particularly in low-resource settings.
SH: What lessons do you think registries in the US can learn from international registries?
FM: International registries often operate in challenging environments, which drives creative and resourceful approaches to cancer surveillance. One key takeaway is how much can be accomplished with limited infrastructure when systems are designed to be practical and efficient. For example, many international registries use streamlined data collection focused on core variables, paired with strong community and institutional partnerships to ensure data completeness.
Another important takeaway is how fragile data systems become without stable funding. Even well-established registries can struggle to maintain quality and continuity when the support is inconsistent. It’s a reminder for the U.S. to continue investing in sustainable registry infrastructure.
On a personal note, when I worked at the São Paulo cancer registry, I often felt intimidated by the scale and sophistication of cancer surveillance in the U.S. I didn’t imagine there would be space for collaboration. But now that I work here, I’ve seen how much the U.S. values and supports international data sharing. There’s a real willingness to learn from other countries and to offer help, and I’ve experienced a level of support and openness that I never expected. That kind of global exchange truly strengthens the field—for all of us.
To learn more about NAACCR’s work with international registries, click/tap on the button below.
What to Read Next

An Interview with Our New RDU Chair
An Interview with our new Research and Date Use Committee Chair It was so much fun interviewing the RDU Co-Chairs…
Sharing NAACCR Pediatric Cancer Initiatives on Dr. Rick Greene’s Cancer Registry World Podcast
I am excited to share that I was recently interviewed by Dr. Rick Greene for his Cancer Registry World podcast….

The Importance of Professional Certification for Cancer Registrars
Professional certification plays a vital role in strengthening the cancer registry workforce and ensuring the high-quality data that is essential…